Dental DSO vs Independent Practice for Growing Dentists
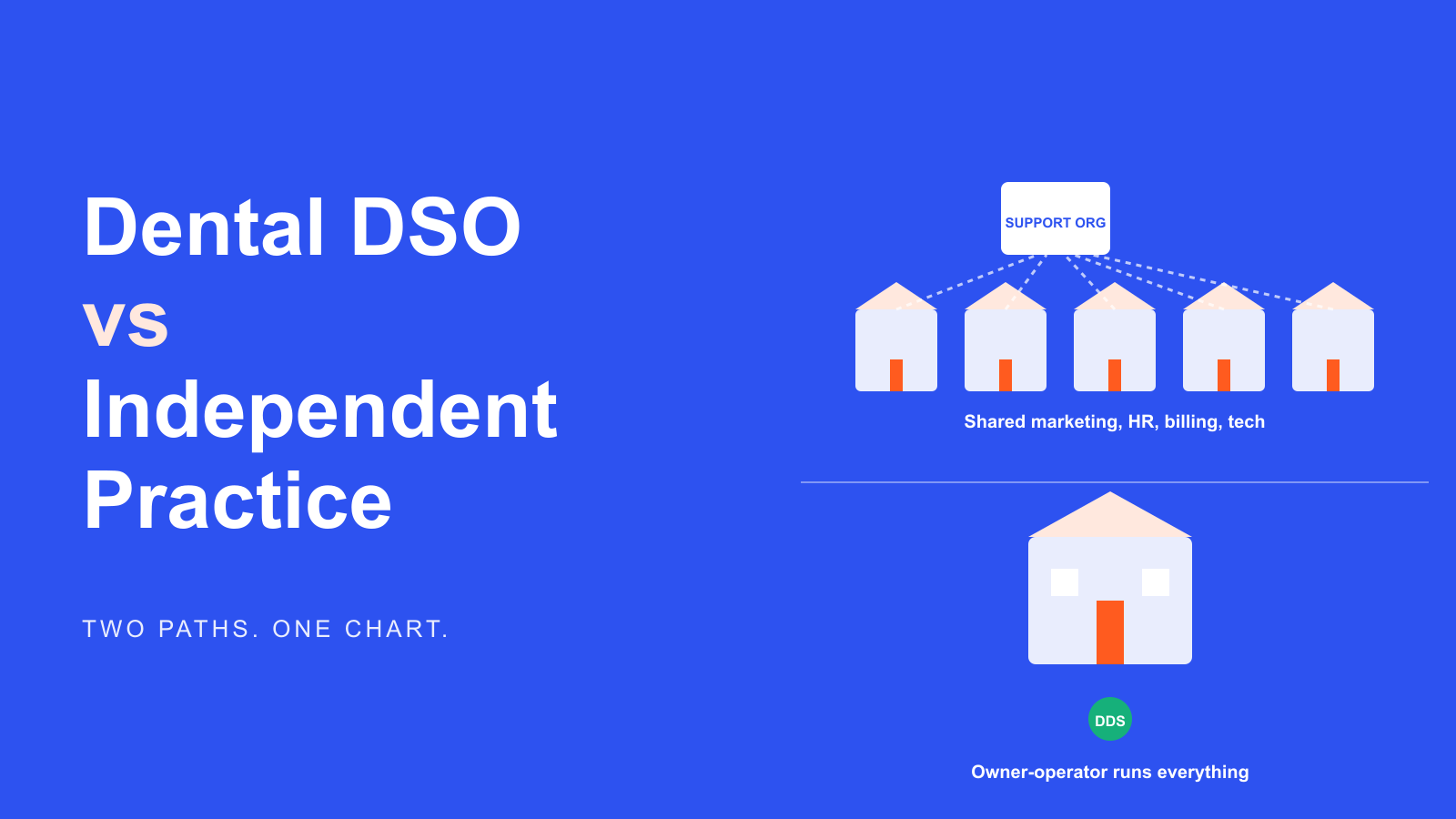
- A dental DSO owns marketing, HR, billing, IT, and administrative functions across a network of affiliated clinics, and the licensed dentist at each clinic keeps clinical autonomy.
- An independent dental practice keeps all of those operating functions under one owner-dentist and their office manager, which trades scale for reaction speed.
- Marketing on a DSO runs at network cadence on quarterly cycles. Marketing at an independent practice runs on weekly cycles with the owner making the calls.
- Sellers evaluating a DSO offer should model equity roll timing, management fee drag, and non-compete geography before signing anything else.
- Smile Design Dentistry ran a 50+ location network that grew PPC conversion rate 20% and cut cost-per-call 30% under a rebuilt central marketing stack, the DSO advantage delivered well.
Ask ten dentists whether they’d sell to a dental DSO and you’ll get ten different answers. Some see it as an early retirement plan. Others see it as losing the practice they spent twenty years building. Both groups usually have the same gap: they’ve never sat down and compared what a dental DSO actually does day-to-day against what an independent dental practice looks like from the inside. That comparison is what this guide walks through. Not the sales pitch from either side. The real operating differences that show up in payroll, patient flow, marketing budgets, and the P&L at year end.
What a dental DSO actually is
A dental DSO is a support company that owns the non-clinical side of a network of affiliated dental practices. The clinical work, the drilling and diagnosis and treatment planning, stays with the licensed dentist at each clinic. The parent DSO handles the rest. Marketing, HR, payroll, billing and revenue cycle, IT, procurement of supplies, real estate, and the reporting layer that rolls up every clinic’s numbers into one dashboard for the executive team. For a longer walkthrough see our guide to the dental service organization operating model. The full dental DSO business model post walks through the fee, roll-up, and rebate math.
The five names most people can list are Heartland Dental, Aspen Dental, Pacific Dental Services, Smile Brands, and MB2 Dental. Behind those five sit several hundred more regional and mid-market DSOs that never make the trade press. Some are private-equity backed. Some are dentist-founded and dentist-run. The structure varies. The premise doesn’t. Concentrate the boring, expensive, hard-to-hire-for functions in one back office and let each clinic focus on patients.
An independent dental practice is the opposite structure. One clinic, sometimes two or three under the same owner-dentist, that runs its own everything. The owner is the CEO, the head of dental marketing, the head of HR, and the primary provider. A good office manager takes on payroll, insurance verification, and vendor relationships. The dentist covers the rest between operatory turnovers.
Ownership structure and the equity question
The single largest difference between a dental DSO and an independent practice is who owns the equity. In an independent practice the dentist owns 100% of the clinic. Every dollar of profit after payroll and overhead belongs to the owner. When the practice is sold, the seller keeps the full sale price minus fees and taxes.
In a dental DSO the structure changes. Most transactions look like this: the DSO buys 70% to 100% of the practice at a multiple of adjusted EBITDA, and the seller rolls a portion of the sale price back into DSO equity. The seller stays clinical for three to five years under an associate agreement, keeps a smaller share of the clinic’s ongoing profit, and holds equity in the parent company that they hope will appreciate before the next recapitalization event. State corporate-practice-of-dentistry laws vary, so most DSOs are structured as a management services organization tied to a professional corporation owned by licensed dentists. The mechanics look complicated on paper. The economics are straightforward once you sketch the flow.
Marketing runs very differently on each side
This is the operating gap most sellers don’t see coming until year two under a DSO. A dental DSO runs marketing at the network level. A central team owns the brand, the paid search accounts, the paid social accounts, the website platform, the review-collection workflow, and the CRM. Each clinic gets a local page under the brand domain, a Google Business Profile that the central team manages, and a monthly budget allocation set by the network, not the clinic owner.
An independent practice does the opposite. The owner picks the vendor, sets the budget, approves the ad copy, and decides which channels to fund, whether that’s Google Ads, Meta, or a full dental ads mix. That control is expensive when you get it wrong. It’s a real asset when you get it right, since the owner can shift budget the same day a channel underperforms. A DSO network cannot move that fast. Central teams work on quarterly cycles, and a per-clinic budget change usually needs a market-manager sign-off and a data pull.
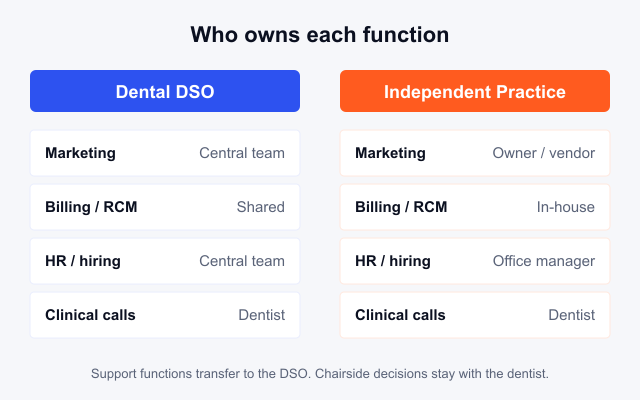
The comparison table below is the frame we use with dentists who are weighing an offer. It’s a snapshot of a typical mid-market DSO against a well-run single-location independent practice with a healthy new-patient flow.
| Function | Dental DSO | Independent practice |
|---|---|---|
| Marketing budget owner | Central team, quarterly cycle | Owner-dentist, weekly cycle |
| Ad account access | Read-only for the clinic | Full admin |
| Website platform | Shared network platform, locked template | Custom, owner picks the CMS |
| Google Business Profile | Managed by central team | Managed by owner or office manager |
| Review collection | Automated at the network level | Manual, staff-driven follow up |
| Patient CRM | Shared instance across clinics | Standalone, tied to the PMS |
| Local sponsorships | Approved from the network budget | Owner writes the check |
| Clinical scope | Full autonomy at the chair | Full autonomy at the chair |
The bottom row matters. Both structures leave the clinical decision to the dentist. The dispute is about who controls everything that happens before the patient sits in the chair.
New-patient economics and per-clinic performance
Growth economics look different at the two structures. A dental DSO tracks new-patient cost of acquisition across the whole network and can spread ad spend over 20 to 50 clinics. That scale gives them lower unit CAC on paid search and paid social. A typical top-quartile DSO reports blended new-patient CAC in the $85 to $140 band across the network, with high-volume clinics well below that and low-volume clinics well above.
An independent practice has none of that scale. It compensates with tighter targeting. When Delicate Dental Group launched its scratch practice, the owner ran the entire local paid-search and Google Business Profile playbook alongside a review generation workflow tied to the PMS. Within twelve months the clinic was pulling 90+ new patients a month at a blended CAC that beat what most DSO clinics in the same market posted, in large part since the owner could react to a low-performing week the same day the report landed. A DSO market manager reviewing the same data usually sees it two weeks later, with three clinics ahead of theirs in the queue for a budget shift. Both structures work. They just move at different speeds.
Provider recruitment and clinical staffing
Recruitment is the other place a dental DSO buys real advantage. A network of 30 clinics can offer a new-grad dentist a signing bonus, mentorship from a lead clinician, benefits, malpractice, and a path to partial ownership through the DSO’s equity program. An independent practice cannot match all of that, or has to stretch to. The trade-off is that DSO associate agreements often lock the dentist into non-competes across a wide radius and revenue-share models that shift compensation with clinic performance rather than personal production.
Independent practices tend to attract dentists who want operational control fast. Ownership track in five to seven years, a smaller team, and a P&L they can see line by line. That model works for a slice of the profession. It doesn’t scale, and hiring cycles are longer since the owner is doing the recruiting on top of clinical work.
Case study anchor with a real network
The clearest picture of DSO-scale marketing we have inside our own portfolio is Smile Design Dentistry, a Central Florida and Tampa Bay dental support organization built on cosmetic, emergency, and preventive care across 50+ locations. When they came to us their central team was carrying inflated ad spend, poor-quality leads, and limited tracking across the network. We restructured the PPC accounts clinic by clinic, added full-funnel paid social, deployed dedicated landing pages per location, and rebuilt CallRail-driven analytics so the market managers could see which leads booked and which didn’t.
The 24-month numbers came in at +20% PPC conversion rate, -30% cost per call, and coverage held across all 50+ locations without a headcount bump on the central team. That’s the DSO promise done well: the network layer carried the marketing load the individual clinics couldn’t have run themselves, and each clinic reported to the same weekly cadence. An independent practice couldn’t have deployed that stack at 50 locations. A DSO without the operating discipline couldn’t have either. The structure only helps when the central team is actually operating it.
Cash flow and the P&L a seller loses
Sellers who join a dental DSO trade upside for stability. Before the sale the owner keeps the practice’s full profit after their own compensation. After the sale the owner earns a base plus a production bonus, keeps a smaller equity stake in the clinic entity, and holds equity in the parent DSO. The parent DSO takes a management fee off the clinic’s revenue every month. Common fee bands run 6% to 12% of collections, sometimes higher.
Whether that math works for a specific dentist comes down to two variables. First, the clinic’s growth rate under the DSO’s operating model. A DSO that grows collections 15% a year makes the fee band feel small. A DSO that runs flat makes the fee band feel very large. Second, the DSO’s equity outcome. If the parent recaps at a higher multiple in three to five years, the rolled equity can double or triple. If it doesn’t, the seller ends up with a fixed sale price and less of the ongoing profit than they had going in. It’s the same risk profile as any private-equity rollup. The upside is real, and the downside is real.
Patient experience differences that show up in reviews
Patients rarely know whether a clinic is DSO-owned or independent. What shows up in reviews is a small set of operating patterns. DSO clinics tend to have longer appointment slots, tighter reminder cadences, and better payment-plan options tied to the network’s dental website template. Those are network investments the individual clinic couldn’t fund alone. Independent clinics tend to score higher on continuity of care, chair time with the same dentist over years, and the small human touches the owner personally trains staff to deliver.
Neither pattern is universal. A well-run DSO clinic with a stable lead dentist reads exactly like a great independent practice from the patient’s side. A poorly run independent practice with high staff turnover reads exactly like the worst DSO horror-story review. The structure sets the ceiling. Operating quality sets the actual result.
Choosing between the two paths
When a dentist asks us to help them think through a DSO offer we walk them through four questions. First, how much of the current profit is coming from the owner’s personal production versus the associates? A high owner-production clinic loses value fast under a DSO fee model. Second, how much would collections grow under the DSO’s marketing and operations layer in the next three years? Get that estimate in writing with named comparable clinics. Third, what is the seller planning to do with the equity roll if the parent doesn’t recap on schedule? Fourth, is the seller genuinely tired of running the business side, or just tired of one specific problem that a good office manager could fix?
The fourth question catches more sellers than the first three combined. A dentist who’s exhausted by hiring, HR, and marketing sometimes sells to the DSO for those functions, then discovers the same functions still eat their attention under the new structure. If the underlying issue is operational chaos in the owner’s own practice, the DSO isn’t the cure. A better office manager and a real dental marketing retainer usually are.
For dentists on the independent side who want the DSO’s marketing muscle without the ownership trade, the closest substitute is a dedicated dental marketing agency running the full stack. Paid search, paid social, review generation, GBP management, and a per-clinic dashboard. It’s cheaper than a DSO fee, doesn’t touch the ownership, and gives the practice most of the network-level gain on the marketing side.
Frequently asked questions about dental DSO vs independent practice
What is the main difference between a dental DSO and an independent practice
The main difference between a dental DSO and an independent practice is who owns and operates the non-clinical side. A dental DSO owns the marketing, HR, billing, IT, and administrative functions across a network of affiliated clinics, and the licensed dentist at each clinic keeps clinical autonomy. An independent practice keeps all of that under a single owner-dentist and their office manager.
The clinical scope is identical. The dispute is about who owns the operating layer around the chair. That difference drives everything downstream: marketing speed, hiring pipeline, cash flow, and what the practice sells for at the end. A dentist evaluating a DSO offer should map the specific functions they’d hand off and price them individually, not treat the offer as one bundled decision.
How can I tell if a dental practice is part of a DSO
Three signals give it away. A shared brand across multiple locations in the region is the fastest tell. Look at the footer of the clinic’s website for a parent-company name, a corporate address that’s not the clinic address, or language like “part of the [Brand] family of dental offices.” The second signal is a shared Google Business Profile management pattern where every location’s photos, hours, and posts follow the same template.
The third is state-level filings. Most dental DSOs operate through a management services organization and a professional corporation owned by licensed dentists. Search the state’s dental board records or the secretary of state’s business filings for the parent corporate name. If the clinic dentist’s employment agreement lists an MSO or corporate services entity, it’s DSO-affiliated. Solo independents show up in filings under the dentist’s own name or a single-office PC.
Do DSO dentists earn more than independent dentists
Total compensation for DSO-employed dentists tends to sit in the $180K to $300K range for associates and higher for lead clinicians with equity, roughly on par with mid-career independent-associate pay. Independent owner-dentists in the top quartile earn well beyond that when the practice is running well, but they carry all the business risk to get there. The average independent owner sits closer to the DSO associate band once you back out overhead and slow seasons.
The right comparison isn’t W-2 to W-2. It’s total take-home plus equity value over ten years. A DSO equity roll that appreciates 3x pays a very different lifetime number than a flat W-2. An independent owner who sells at year 15 for a real practice value ends up at yet another number. Run all three scenarios before choosing.
Can an independent dental practice compete with a DSO on marketing
Yes, and the smaller practices with a real marketing partner beat DSO clinics in their local market often. The DSO’s advantage is spread across a network. In any single ZIP code the DSO clinic is running the same ad copy, the same landing page, and the same GBP template as its cousin two markets over. An independent practice can out-target that with local specificity, faster review response, and a website built for one market rather than fifty.
What the independent practice cannot match is the media budget. A DSO clinic in a competitive metro often has a $12K to $30K per month paid budget flowing through the central account. An independent practice at $3K to $8K per month wins on efficiency, not volume. That gap closes when the independent works with a specialist team that gets more per dollar than a network buyer running 50 accounts.
What are the biggest risks of joining a dental DSO
The three risks that show up most often are equity roll timing, management fee drag, and non-compete scope. The equity roll only pays if the parent DSO recaps at a higher multiple within the seller’s stay period, and rate cycles have made that timeline less certain since 2022. The management fee reduces the clinic’s ongoing distributions in a way many sellers underweight at signing.
The non-compete is the least discussed and the most binding. Most DSO associate agreements cover a radius of 10 to 25 miles for two to three years post-separation. A dentist who exits earlier than planned finds it very hard to open a competing clinic in the same market. Read the non-compete before signing anything else. If a seller doesn’t feel the DSO is the last stop in their career, negotiate the geography and duration down before agreeing to the sale terms.
How does patient care differ between a dental DSO and an independent practice
Patient care itself does not differ by structure. The same clinical standards, licensing rules, and treatment protocols apply. What differs is the wrapper. DSO clinics tend to run tighter reminder systems, more standardized new-patient onboarding, and better payment-plan options. Independent clinics tend to score higher on continuity of care and personal relationship depth with the same dentist over years.
The variance within each structure is far larger than the variance between structures. A well-run DSO clinic and a well-run independent practice look similar to a patient. A poorly run version of either shows up in the same ways: staff turnover, rushed appointments, and pressure on unnecessary treatment. The patient’s best signal is reviews across at least the last 90 days plus a conversation with a hygienist during a first visit, not the ownership model on the door.
If your practice is weighing an offer or wants to run the independent path with real marketing behind it, see how we help dental marketing teams book more first-visit patients across single and multi-location groups. Our team supports multi-location dental networks on central-account restructures and per-clinic dashboards too, similar to the Canadian Orthodontic Partners rebuild across 65 clinics.
Book your free 30-minute strategy call.
No spam, no sales rep. We use your email to schedule your call with a senior strategist. That is it.
More from the blog
View all articles → Marketing Strategy
Marketing Strategy How Dental DSOs Grow Through Marketing. Tactics That Scale
Read article Marketing Strategy
Marketing Strategy Dental DSO Marketing Services. What to Expect From an Agency Partner
Read article Marketing Strategy
Marketing Strategy