What Does DSO Stand For in Dental in Simple Terms
- DSO stands for Dental Support Organization. Business services only.
- Management fees run 15 to 25 percent of collections.
- About 30 percent of US practices sit inside a DSO in 2026.
- Equity rollover often returns 2x to 3x on a good DSO recap.
- Ask five filter questions before the second call.
- The direct answer to what does dso stand for in dental terms
- The DSO acronym dental owners run into in legal contracts
- Revenue math behind the DSO acronym for dental practice affiliation
- Industry scale after you know what does dso stand for in dental practice
- Culture signals inside the DSO acronym for dental teams
- Marketing side of the DSO acronym dental teams rarely see
- Real DSO case study on the acronym in action
- Questions to answer before the DSO stands for dental affiliation makes sense
- Common myths worth clearing after the DSO acronym conversation
- Where to start once the DSO acronym for dental affiliation intrigues you
What does dso stand for in dental industry conversations is the shortest acronym question with the longest business answer. DSO stands for Dental Support Organization. The DSO is the corporate entity that runs the non-clinical side of a dental practice or a group of practices, while the clinical work stays under the licensed dentist. Roughly 30 percent of US dental offices already sit inside a DSO in 2026, and the acronym is now everywhere in trade press and recruiter conversations.
This guide is the direct read on what does dso stand for in dental terms for a practicing dentist. You get the acronym breakdown, the structural map, the revenue math, the industry heavyweights by size, the cultural signals worth catching early, and the questions every practice owner should ask before a term sheet lands. Read straight through in about ten minutes and keep the reference tab open for your next recruiter call.

The direct answer to what does dso stand for in dental terms
The answer to what does dso stand for in dental industry usage: DSO stands for Dental Support Organization. Three words. The three cover the model completely. Dental names the industry. Support names the function. Organization names the entity. The DSO delivers business services to affiliated dental practices under a management services agreement, takes a management fee, and lets the dentist focus on chair time. The corporate parent handles marketing, billing, HR, IT, procurement, and compliance across the network.
The DSO acronym dental teams see everywhere replaced the older term dental chain in the mid-2000s. Corporate practice of dentistry laws in most states forced the industry to separate corporate ownership from clinical practice. The DSO structure gave everyone a legal path. The DSO owns the back office. The dentist owns the clinical entity. The MSA bridges the two. That legal workaround is why the DSO acronym now dominates every dental trade publication and every private equity healthcare tracker in the country.
Where the DSO acronym came from
The DSO acronym for dental group support entered the trade press around 2004 to 2006, as state dental boards pushed back on the old chain model. Heartland Dental, Aspen Dental, and Pacific Dental Services helped define the operating template that other DSOs still copy. As private equity funding scaled, so did the acronym. By 2015 every dental trade conference had a DSO track. By 2020 the acronym showed up in mainstream healthcare business news. Today the DSO acronym is standard terminology in every corner of the industry.
The DSO acronym in day-to-day practice
The DSO acronym dental owners hear at recruiter events maps to specific operating changes on the ground. Marketing runs from a central team. Billing runs through a shared RCM group. HR handles hiring and benefits. IT patches the practice management software. Procurement gets bulk discounts on supplies. The regional operations manager visits the office on a rotation and sits with the owner on strategy calls. Every one of those changes flows from three words on a business card. Dental. Support. Organization.
The DSO acronym dental owners run into in legal contracts
To fully understand what does dso stand for in dental legal contracts: every DSO deal names the corporate parent as the DSO entity and the practice as the professional corporation or PC. The management services agreement between the two spells out the DSO acronym meaning in legal terms. The DSO provides business services listed in a service exhibit. The PC pays a management fee tied to collections. The DSO does not touch clinical decisions. The PC does not touch marketing budget or HR policy. Each side stays in its lane by contract, not by handshake.
The DSO acronym for dental legal purposes carries specific weight in states with strict corporate practice laws. Texas, California, New York, and about 30 other states forbid non-dentists from owning a dental practice. The DSO structure keeps the corporate parent out of clinical ownership and keeps the model legal. A dental chain that violated those rules gets shut down. A DSO structured properly stays operating for decades. Study the ADA News coverage on how state boards enforce these rules.
| Element | DSO parent | Practice PC | Contract layer |
|---|---|---|---|
| Owner | Corporate LLC or Inc | Licensed dentist | Management Services Agreement |
| Handles | Marketing, HR, IT, RCM | Clinical care | Term, fees, exits |
| Legal status | Non-clinical entity | Regulated dental practice | Enforceable both ways |
| Revenue source | Management fee | Patient collections | Fee formula |
Legal boundary between the entities
The DSO cannot legally direct clinical treatment. The dentist cannot legally reassign marketing or billing without amending the MSA. Both boundaries protect both sides. When a DSO oversteps and tells a dentist which procedure to recommend, the practice board complaint gets filed and the DSO loses on the enforcement action. When a dentist tries to run corporate marketing themselves without notifying the DSO, the MSA gets amended or the affiliation ends. Read the boundary sections of the MSA carefully. That is where the friction lives.
Contract term and renewal mechanics
Most MSAs run 20 to 40 years with automatic renewal options. That length shocks dentists coming from solo practice. The rationale is the long payback horizon on the DSO investment, especially the equity rollover math. Read the renewal clauses. Read the termination clauses. Read the noncompete radius that applies if the affiliation ends. A 40-year term with a five-county noncompete radius restricts your options if the DSO fails. A 20-year term with a two-county noncompete radius keeps more flexibility open. Term length matters more than most dentists initially recognize.
Revenue math behind the DSO acronym for dental practice affiliation
Once you understand what does dso stand for in dental terms, the revenue math becomes the real study. Take a $2 million per year practice affiliating with a mid-tier DSO. The DSO takes a 20 percent management fee, moving $400,000 up the chain. Clinical overhead runs 45 percent, or $900,000. Owner dentist compensation, at 30 percent of collections, is $600,000. The remaining $100,000 stays in the practice as reserve cash for equipment replacement and unexpected expenses.
The equity rollover is where the real DSO math lives. Most affiliation deals ask the selling dentist to roll 20 to 40 percent of sale proceeds into DSO parent equity vesting over two to five years. If the DSO doubles enterprise value and sells to a larger PE firm at a higher EBITDA multiple, that rolled equity often returns 2x to 3x. On a $2 million practice with a $2.5 million transaction value at a 6x multiple, a 30 percent rollover of $750,000 might return $1.5 million to $2.25 million on the next recap event.
Fee formulas vary more than the headline suggests
Some DSOs charge a straight percentage on collections. Others structure a lower percentage plus a fixed dollar amount per operatory. Others build a graduated formula that drops the percentage if the practice hits growth targets. A 20 percent flat fee looks similar to a 15 percent plus $2,000 per chair formula until you run the year-three math and the numbers diverge by $60,000 annually. Ask for the formula in writing. Model three years forward. Compare across three DSOs before you name a preferred structure.
Compensation structure worth negotiating
Owner dentists in affiliation deals earn 30 to 35 percent of collections plus DSO parent equity vesting over the term. Associate dentists earn a base salary of $150,000 to $220,000 plus a production bonus of 25 to 30 percent above a daily threshold. Some DSOs cap production comp at a ceiling. Others let it run. The comp structure matters more than the headline number. A high base with a low ceiling caps earnings on a strong year. A lower base with an open ceiling rewards you during peak seasons.
Every DSO conversation lives or dies on the Management Services Agreement, not the sale price. Ask for a sample MSA on the first call, not week five.
Industry scale after you know what does dso stand for in dental practice
Once you know what does dso stand for in dental practice terms, industry scale becomes the next question. Roughly 400 to 500 DSOs operate in the US in 2026, running about 12,000 to 14,000 dental practices. That number is close to 30 percent of the total practice count. Five years ago the number sat at 18 percent. Ten years ago it was 12 percent. The trend line is steep and shows no sign of slowing through the rest of the decade.
Heartland Dental runs about 1,700 offices across 38 states. Aspen Dental Management runs about 1,000. Pacific Dental Services runs about 950. Smile Brands, Great Expressions Dental Centers, MB2 Dental, and Dental Care Alliance each run several hundred. Together the top 10 DSOs cover about 6,000 practices, close to half of the DSO segment total. The tail sits at about 400 mid-tier DSOs running 15 to 60 offices each. Most affiliation conversations happen in that mid-tier segment.
- Heartland Dental at about 1,700 offices across 38 states
- Aspen Dental Management at about 1,000 offices
- Pacific Dental Services at about 950 offices
- Smile Brands, Great Expressions, MB2 Dental at several hundred each
- Dental Care Alliance, InterDent, Riccobene at 100 to 300 offices
- Mid-tier tail of 400 DSOs at 15 to 60 offices each
- Small specialty DSOs in ortho, pediatric, and oral surgery segments
The mid-tier DSO where most deals close
Mid-tier DSOs run 15 to 60 offices, typically under private equity ownership, and typically planning to sell to a larger PE firm inside three to five years. That segment is where equity rollover math tends to deliver the strongest returns because the DSO still has growth ahead of it. The tradeoff is that mid-tier DSOs have less operational maturity than the top platforms. Culture varies practice by practice. Regional manager tenure varies. Ask for three named references at practices your size before you sign anything with a mid-tier DSO.
Specialty DSOs and their higher multiples
Specialty DSOs in orthodontics, pediatric dentistry, oral surgery, and endodontics pay higher acquisition multiples than general dentistry DSOs. Referral flow, case value, and payer mix in those specialties each carry more predictable economics. Smile Doctors runs the largest ortho DSO with several hundred offices. Pediatric platforms like Smile Design and Chompers run similar rollups. A specialist thinking about affiliation should ask for specialty comparables, not general dentistry data. The multiples differ enough to shift the entire deal math.
Culture signals inside the DSO acronym for dental teams
The what does dso stand for in dental practice answer is the same for every group, but two DSOs can share the same acronym and run completely different operating cultures. One might be dentist-founded with a slow growth model and strong clinical judgment. Another might be PE-backed with aggressive quarterly production targets. Same three-letter acronym. Opposite operating culture. Every affiliation decision hinges on the specific DSO, not on the general DSO category. Ask affiliated dentists off the record. Ask what happens when a practice misses a monthly production target twice in a row. That answer tells you the whole culture in one sentence.
Look at three signals. First, ownership structure and time since the last recapitalization event. A DSO one year into a new PE cycle behaves differently than one four years in. Second, regional manager tenure in your area. Regional managers who stay three years build real relationships. Regional managers who cycle every 18 months treat practices like line items. Third, marketing execution across the network. A DSO whose per-office paid media reports are unavailable or unimpressive is a DSO whose entire operating model may be equally shallow. See HubSpot on multi-location marketing for the operational tension every group runs into once scale kicks in.
PE-backed vs dentist-led DSOs
PE-backed DSOs move fast. Growth targets get set quarterly. Acquisitions happen monthly. Marketing gets funded generously. Regional managers cycle every 18 to 24 months. Dentist-led DSOs move slower. Growth is deliberate. Regional manager tenure runs longer. The tradeoff for dentist-led DSOs is less capital and slower operational maturity. Neither model is inherently right or wrong. The correct choice depends on whether you want speed and scale or continuity and slower growth. Match the DSO model to your own five-year plan for your practice.
Production culture reveals the DSO on day one
The clearest culture signal shows up in how the DSO talks about production. A DSO that leads with clinical outcomes and patient satisfaction is telling you where their focus sits. A DSO that leads with monthly production targets and quarterly quotas is telling you the same from the other side. Neither is inherently wrong. Both cultures work for different dentists. Just make sure the culture you sign into matches how you actually want to practice for the next five to ten years, not just the next quarter.
Marketing side of the DSO acronym dental teams rarely see
The marketing side of the DSO acronym dental teams rarely see up front decides a large share of the value delivered. A DSO with a working marketing stack pulls 20 to 40 percent more new patients per location than a comparable solo practice. A DSO with a broken marketing stack costs the affiliated dentist 15 to 25 percent of the new patient volume they would have generated solo. Marketing execution is the single largest hidden variable in DSO economics.
Working stacks share five features. Shared brand equity across locations with per-location subpages that carry local trust cues. Google Business Profile management run by someone who has worked map pack rankings before. Location-specific paid search built at the office level, not the metro level. Awareness and consideration paid social layered across the market. And call tracking that scores every ring by whether it booked. Skip any one and the new patient count underperforms across the network. See our dental SEO services writeup for the full breakdown.
Per-location detail that decides map pack rankings
Map pack rankings live on office-level detail. Named front-office manager on the location page. Real staff photos, not stock. Neighborhood mentions the local search index picks up. Reviews collected office by office with real patient names. Citations in the same NAP format across every directory. Every one of those is per-location work. A DSO marketing team that treats 40 offices as one program cannot deliver map pack coverage. A DSO marketing team with per-office ownership can deliver it every quarter.
Call tracking as the truth layer
Call tracking is the single feature that separates a real DSO marketing program from a spreadsheet exercise. Every call scored on booked or not booked. Every source tagged. Every campaign judged on cost per booked new patient. A DSO without call tracking has no way to defend its marketing budget on a board call. A DSO with call tracking can rebalance spend across offices weekly and push budget to the markets returning the strongest new patient numbers. Non-negotiable at scale.
Every dentist who signs a DSO deal remembers the branded fleece. Every recruiter shows up wearing a branded fleece with the DSO logo embroidered on the chest. Every meeting starts with talk about culture and community. Every closing packet ships with a matching branded fleece for you and one for your spouse. The fleeces are actually pretty comfortable. Then you read the term sheet at 11 pm on a Wednesday, notice the noncompete radius covers three counties, and try to reach the rep whose branded voicemail is now full.
Real DSO case study on the acronym in action
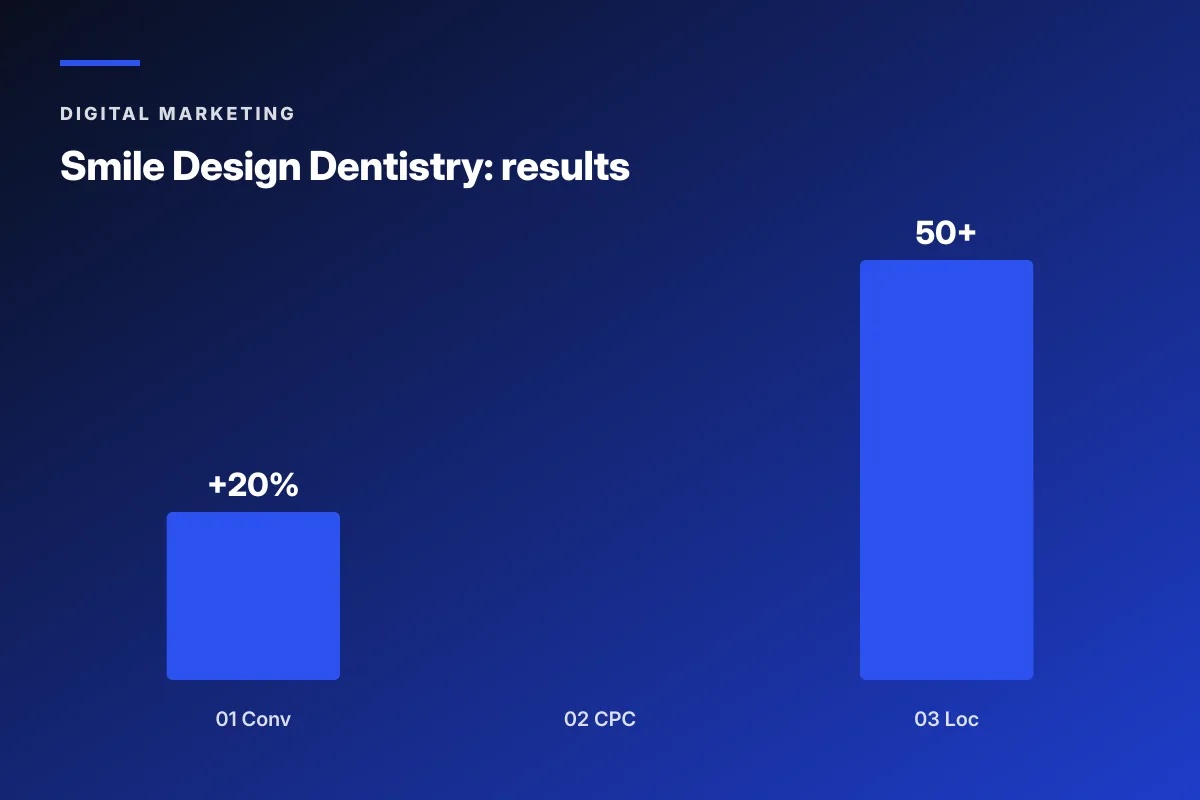
Smile Design Dentistry, a 50-plus location DSO based in Central Florida and Tampa Bay, showed us what does dso stand for in dental operations at scale. The DSO faced the same problem every mid-size DSO faces at scale. Ad spend up. Patient quality down. PPC campaigns targeting too broadly. Landing pages that could not close a phone-in visitor. Paid social barely used. Tracking thin enough that the executive team could not tell which office pulled the strongest paid media performance in any given month.
We ran a per-location, per-funnel-stage rebuild. Google Ads got restructured by geo and by intent stage. Landing pages got built for each office with local trust cues layered under a national brand system. CallRail integration scored every call by patient quality, not just call volume. Paid social launched with awareness, consideration, and conversion layers built to move a prospect through the funnel with video and demographic precision. PPC conversion rate gained 20 percent. Cost per call dropped 30 percent. All 50-plus offices got optimized campaigns instead of a shared template.
Stack detail that moved the numbers
Funnel-stage campaign structure. Geo-modified bid targeting at the office level. Landing pages that named the neighborhood, the front office manager, and the two closest cross streets. Call scoring on every ring. Weekly reporting by office. Ongoing creative testing with capacity-aware budget allocation. Every one of those pieces reinforced the next. Skip the call scoring and the paid media dashboard turns into a vanity report. Skip the landing pages and the paid clicks bounce. Skip the reporting cadence and budget stays trapped in low-return markets for months.
Lessons for any DSO at scale
The Smile Design playbook translates cleanly to any DSO running 10-plus offices in a shared media market. Per-location landing pages with local trust cues. Call scoring on every ring. Funnel-stage campaign structure. Weekly per-office reporting. Skip any one of them and the paid media budget grows every quarter without moving new patient counts. Every dentist considering DSO affiliation should ask for three months of per-location paid media reports before signing anything. See our DSO dental marketing for multi-location groups writeup for the full rollout pattern.
Questions to answer before the DSO stands for dental affiliation makes sense
The DSO stands for dental affiliation option makes sense only after you answer three questions honestly. First, how long do you plan to keep practicing chairside. If retirement sits inside a decade, DSO timing matches your exit. Second, do you want to grow past a single location. If yes, DSO capital moves you faster than solo growth. Third, how much clinical autonomy do you need to stay happy. If losing 15 percent of operational calls would wreck your Monday, no term sheet is worth signing.
Practices most likely to be happy inside a DSO are producing $1.5 million to $6 million a year, run three or fewer operatories, want out of operational headaches, and have an owner within ten years of retirement. Practices most likely to regret a DSO deal are producing under $900,000, run heavy specialty procedures the DSO does not staff for, or have a strong personal-brand owner whose patients would not stay after the sale. The fit question is about the practice, not the DSO.
Preparation before the first DSO call
Read your last three years of tax returns before you talk to a DSO. Know your EBITDA. Know your collections trend. Know your patient count. Know your production per hour. Know your insurance write-off percentage. If you cannot recite those numbers, you are not ready to negotiate. DSO reps are trained to walk you through their preferred multiple. Your preparation is the only counterweight. Get your accountant to run a quality-of-earnings analysis before you sign anything. That report costs about $8,000 and saves ten times that in the negotiation.
What to expect after you sign
The first 90 days after closing are the hardest. The DSO drops its operating manual on your team. Your practice management software may switch. Your uniforms may change. A regional manager visits every week. Some team members quit. Others rise. Marketing budget moves from your local vendor to the DSO central team. Patient reactions vary. Most patients notice nothing. Some ask why the front desk voicemail changed. Give the transition a full year before you judge the deal. The rough patches usually smooth out. The permanent changes are worth knowing about in advance.
Common myths worth clearing after the DSO acronym conversation
Once a dentist studies the DSO acronym seriously, a handful of persistent myths deserve a reality check. Myth one: DSOs always overwork their dentists. Reality: some do, most run the same production expectations as a healthy solo practice, and the culture varies by group. Myth two: every DSO offer is the same. Reality: fee formulas, comp structures, and equity terms vary widely across three DSOs in the same negotiation.
Myth three: the equity rollover is a scam. Reality: strong DSOs deliver real returns to affiliated dentists on recap events. Weaker DSOs do not. Myth four: you cannot leave a DSO. Reality: MSAs have termination clauses that spell out exit conditions clearly. Myth five: patients notice the affiliation. Reality: most patients notice nothing beyond a possible change in front-desk voicemail. The reality on all five myths is more nuanced than industry Twitter suggests. Study each one before you buy or dismiss it.
Why the myths persist despite the data
Industry forums surface strong opinions faster than balanced data. A single bad affiliation experience gets written up in detail. A hundred smooth affiliations stay quiet. The result is a public conversation weighted toward horror stories. That skew is worth remembering when you read online debates about DSOs. Real data on affiliation outcomes comes from the DSO trade groups and from PE firm quarterly reports, and both sources tell a more balanced story than the loudest forum posts imply.
Taking a balanced view before deciding
A balanced view weighs the specific DSO in front of you against the specific alternative path you have. Solo growth is a real option. Slower expansion under a group practice partnership is another. Selling to a private buyer instead of a DSO is a third. Each path has math worth running. The DSO decision is one option among several, not the default endpoint for every dentist. Treat it that way and the choice you make sits on better ground.
Where to start once the DSO acronym for dental affiliation intrigues you
If the DSO acronym for dental affiliation intrigues you enough to explore, start with three specific actions. Pull three years of tax returns and prepare a quality-of-earnings package. Talk to three DSOs and collect comparable term sheets. Talk to two affiliated dentists inside each DSO off the record. Those actions cost you nothing but time and set up the negotiation cleanly. Rushing past them costs you five to ten percent of the sale price on average across the deals we have watched.
Once the term sheets arrive, involve a transaction attorney familiar with DSO deals. Compare fee structures, comp formulas, equity rollover terms, noncompete radii, and exit clauses side by side. If two DSOs come in inside a 10 percent band, the deal is fair. If one is 25 percent above the others, ask why. If one is 25 percent below, walk. Ready to look at what a real dental marketing program covers as an alternative to affiliation, our dental marketing agency hub covers the full engagement. For the retainer math, our dental marketing retainer writeup covers what a growth practice pays for a working stack. And Google Search Central is the reference for schema markup a DSO site should carry across every location.
Three-action checklist for the next 30 days
Pull tax returns for the last three years. Prepare a quality-of-earnings package with your accountant. Book intro calls with three DSOs. Ask each rep the five filter questions on the first call and note answers verbatim. Rank the three DSOs on culture, execution, and math. Talk to two affiliated dentists inside each of the two finalists off the record. That thirty-day sequence gives you enough information to know whether to move forward or walk. And the same thirty days gives you the pull at the table you would otherwise miss.
Decision check at day 30
At day 30, ask yourself three questions. Does the top DSO offer feel financially fair after seeing three side by side. Do you trust the operating culture based on the affiliated dentist references you spoke with. Can you live with the clinical autonomy tradeoff for the term of the MSA. If all three answers are yes, move forward with letter of intent. If any one is no, walk or take another sixty days to explore. The decision is one of the biggest of your career. Take the time it deserves.
Frequently asked questions
What does DSO stand for in dental practice terms exactly
DSO stands for Dental Support Organization. It is the corporate entity that runs the non-clinical side of a dental practice or a group of practices under a management services agreement with the licensed dentist. Marketing, billing, HR, IT, procurement, real estate, compliance, and finance sit inside the DSO. The clinical work and the dental license stay with the dentist. That structure keeps the arrangement legal under state corporate practice of dentistry laws in the roughly 30 states that require a licensed dentist to own any dental practice entity. The DSO earns a management fee, usually 15 to 25 percent of collections.
What does DSO stand for dental industry uses versus older terms like dental chain
The DSO acronym replaced the older term dental chain in the mid-2000s once state dental boards pushed back on the chain model. A dental chain owns every office directly and employs every dentist as W-2 staff. A DSO keeps clinical ownership in the hands of a licensed dentist and runs business services under a management services agreement. Same corporate dentistry category. Different legal structure. The DSO structure keeps state corporate practice laws satisfied and lets private equity fund the space at scale. Today the DSO acronym dominates every dental trade publication and every private equity healthcare tracker.
How does DSO stands for dental translate to practice-level economics
When DSO stands for dental practice affiliation, the economics land in four numbers on a real practice. Take a $2 million per year practice. The DSO takes a 20 percent management fee, so $400,000 goes up the chain. Clinical overhead runs 45 percent, or $900,000. Doctor compensation at 30 percent of collections pulls $600,000. The remaining $100,000 stays in the practice as reserve cash. The equity rollover on affiliation adds a separate upside track that often returns 2x to 3x on a good DSO recap. Downside cases exist too and deserve equal review before signing.
What does the DSO acronym dental teams use mean in day-to-day practice
The DSO acronym dental teams hear at recruiter events maps to specific operating changes on the ground. Marketing runs from a central team. Billing runs through a shared revenue cycle management group. HR handles hiring, benefits, and payroll. IT patches the practice management software. Procurement gets bulk discounts on supplies. A regional operations manager visits the office on a rotation and sits with the owner on strategy calls. Every one of those changes flows from three words on a business card: Dental Support Organization. The acronym translates directly into how the office runs after affiliation.
How is the DSO acronym for dental group affiliation different from corporate dentistry
Corporate dentistry is the umbrella category for any commercial ownership structure in dentistry. It includes DSOs, publicly traded chains, insurance-owned practice groups, and private equity platforms. A DSO is one specific model inside that category, defined by a management services agreement between a corporate parent and a dentist-owned practice PC. Every DSO is corporate dentistry. Not every corporate dental group is a DSO. The distinction matters when reading industry news, evaluating an acquisition offer, or explaining the model to team members and patients after affiliation. Get the terminology right before entering any negotiation.
Which DSOs are the largest and what does the tail look like
Heartland Dental runs about 1,700 offices across 38 states. Aspen Dental Management runs about 1,000. Pacific Dental Services runs about 950. Smile Brands, Great Expressions, MB2 Dental, and Dental Care Alliance each run several hundred. Together the top 10 DSOs cover about 6,000 practices, close to half of the DSO segment total. The tail sits at about 400 mid-tier DSOs running 15 to 60 offices each, typically PE-owned and planning to sell inside three to five years. Most dentists thinking about affiliation end up talking to a mid-tier DSO, not one of the giants.
Book your free 30-minute strategy call.
No spam, no sales rep. We use your email to schedule your call with a senior strategist. That is it.
More from the blog
View all articles → Digital Marketing
Digital Marketing Dental Marketing Tips That Compound Into New Patients
Read article Digital Marketing
Digital Marketing Ecommerce Marketing Strategies That Drive Real DTC Revenue
Read article Digital Marketing
Digital Marketing