Healthcare Website Development and What Practices Actually Need to Build
- Healthcare website development covers compliance, security, and integrations.
- CMS choice locks the next five years of maintenance profile.
- HIPAA-compliant hosting with signed BAA is a baseline, not a premium add.
- Every form that touches PHI needs encrypted submission and a signed BAA.
- Performance budgets locked at day one beat later optimization every time.
- What Healthcare Website Development Actually Covers
- Healthcare Web Development Common Requirements
- Web Development for Healthcare and the CMS Decision
- Healthcare Web Application Development and Custom Portals
- Comparing Healthcare Website Development Stacks
- Security, Forms, and Analytics in Healthcare Development
- Healthcare Web App Development and Real Integrations
- Healthcare Website Development Case Study From a Real Client
- Hosting, Backups, and Ongoing Development
- Performance Budgets and Core Web Vitals in Development
- How to Scope Healthcare Website Development Correctly
Healthcare website development is the layer that most stakeholders never see and every stakeholder eventually pays for. Design carries the brand. Development carries the compliance, the security, the integrations, the forms, the analytics, and the reason the site still runs a year after launch without exposing patient data. Skip a requirement and you either pay to rebuild in six months or you accept a legal exposure the practice cannot afford. This guide walks through what actually gets built when a healthcare website goes into development, what the common requirements look like in a real project, where the hidden costs live, and how the decisions in this phase constrain everything design has already committed to. If you are the practice owner, the marketing lead, or the office manager who signs the invoices, this is the piece to read before the developer starts writing code, because most of the expensive mistakes are made here.
What Healthcare Website Development Actually Covers
Healthcare website development covers the working stack behind the design. CMS setup, form architecture, hosting configuration, security hardening, and third-party integrations. It also covers accessibility implementation, performance budgets, analytics setup, and the QA passes that decide whether the site launches on time.
Every one of those items is a design constraint in disguise, and every skipped item shows up as a bug three months after launch. The practice does not have to become an expert. It does have to understand which decisions live in this layer.
Why development scope creeps
Healthcare development projects almost always creep because the practice discovers integration and compliance requirements the discovery call missed. The insurance portal that has to embed. The EHR system that has to talk to the booking form. The pharmacy tie-in that nobody mentioned until the doctor asked. Each of those adds days to the estimate. A working discovery process catches most of them up front, but no discovery catches all of them, so a healthy budget line for scope contingency belongs in every healthcare development quote.
Why development is where compliance actually lives
Design produces the layouts. Development produces the compliance. HIPAA, ADA, WCAG, and every relevant state privacy rule get enforced or ignored in the code, not in the wireframe. Practices that treat development as a commodity phase end up with beautiful designs riding on non-compliant plumbing. That is the fastest path from launch celebration to legal letter.
Why development scope decides the retainer
The complexity of the development phase decides how much ongoing maintenance the site will need. A custom-coded booking flow with three third-party integrations needs monthly attention. A well-configured off-the-shelf stack needs quarterly attention. Neither is inherently better, but the decision made during development commits the practice to a retainer shape for years.
Healthcare Web Development Common Requirements
Healthcare web development has a common requirements list that repeats across almost every practice we work with. Solo primary care, multi-provider clinic, multi-location network, specialty group, telehealth-first. The details change. The requirements do not. Here is the working list every quote should cover, because if it is not in the scope document, it is not in the build.
- CMS that the practice can update without a developer for basic content changes.
- Form stack with encrypted submission and a signed BAA with the vendor.
- HIPAA-compliant hosting environment with signed BAA and enforced HTTPS.
- Analytics implementation that does not capture protected health information.
- Booking flow that integrates with the practice’s actual scheduling system.
- Accessibility features built to WCAG 2.1 AA baseline across every template.
- Core Web Vitals passing at the 75th percentile of mobile traffic.
- Backup and disaster recovery configured with off-site copies and tested restores.
- Security hardening including WAF, rate limiting, and CMS user role audits.
- Third-party integrations documented so future developers can maintain them.
The item most healthcare quotes silently skip
Backup and disaster recovery is the item that gets skipped or hand-waved in most healthcare development quotes. Agencies tend to assume the host handles it. Hosts tend to assume the agency handles it. Neither actually configures it end-to-end unless the practice asks. The first time the site has a database issue, everyone learns whose responsibility it was. The practice pays for the education.
Why the CMS choice locks the next five years
The CMS decision is one of the highest-impact choices in the whole project. WordPress with a HIPAA-compatible host, a headless setup with Next.js, or a specialty platform like Weebly Health each carry different maintenance profiles, plugin ecosystems, and developer availability. Best-in-class development picks the CMS that matches the practice’s internal capacity for updates, not the CMS the developer prefers to work in.
Why integrations dominate the timeline
Every healthcare site has integrations. Scheduling systems, insurance verification, EHR platforms, pharmacy tie-ins, review aggregators, patient portals. Each integration adds a discovery step, an authentication flow, a data mapping exercise, and a QA loop. The design might be done in four weeks. The integrations often take six.
Web Development for Healthcare and the CMS Decision
Web development for healthcare has to start with a CMS decision that survives the next five years. Practices routinely make this call based on what the current developer prefers, and that is almost always the wrong reason. The right reason is a match between the practice’s internal capacity, the site’s integration needs, and the plugin or module ecosystem available for healthcare-specific requirements.
WordPress in healthcare
WordPress runs about 40 percent of the healthcare sites we audit. It has the widest plugin ecosystem, the largest developer pool, and the deepest history of accessibility and security modules. It also has the widest surface area for security vulnerabilities if not maintained. Best-in-class WordPress healthcare setups run a managed HIPAA host, a hardened admin, monthly plugin updates, and a limited plugin roster. Slap-together WordPress setups are the source of most of the healthcare breach headlines.
Headless and JAMstack
Headless setups with a decoupled CMS and a Next.js or Astro front end offer performance and security advantages, but they require ongoing developer availability. Practices that pick headless without securing a long-term developer relationship end up stuck when even minor content changes need code deploys. Headless is the right call when the practice has budget for a monthly retainer with a specialist team and the site needs advanced integrations.
Specialty healthcare platforms
Specialty platforms like Officite, MyAdvice, and Weebly Health offer pre-built compliance and integration features specific to healthcare. They cost more per month than open-source options and lock the practice into the vendor’s roadmap. They also remove the compliance guesswork for smaller practices that lack internal technical staff. The trade-off is flexibility versus overhead. Neither is universally right.
Every EHR, insurance portal, or booking sync adds 2 weeks to build. List every third-party tie before signing the SOW. Nothing hurts scope more than a Week 5 discovery.
Healthcare Web Application Development and Custom Portals
Healthcare web application development is a different category from marketing site development. Custom patient portals, appointment reminders, telehealth waiting rooms, and provider dashboards all involve custom application work with different compliance, security, and maintenance obligations. Practices asking for a website often need parts of an application, and the confusion between the two categories drives most of the budget overruns we see.
When a marketing site is enough
A marketing site is enough when the practice needs a public-facing presence with service information, provider bios, and a booking form that hands off to an external scheduling system. That is 80 percent of what most single-provider and small multi-provider practices actually need. Adding custom application logic to a marketing site scope is where budgets triple without a matching gain in outcomes.
When custom application logic is required
Custom application development becomes necessary when the practice runs multi-step patient intake, custom insurance verification, provider-facing dashboards, or telehealth features that the off-the-shelf tools do not support. Multi-location networks, specialty groups with custom clinical workflows, and DSO-scale operators typically need application development. Solo practices rarely do. The honest scoping conversation separates the two before the quote lands.
The hybrid pattern that works
Most mid-size healthcare projects land on a hybrid. WordPress or a headless CMS handles the marketing content. A separate custom-built application handles patient portal features. The two are connected through an authenticated hand-off. This pattern separates the maintenance responsibilities and keeps the marketing site fast without inheriting the compliance burden of the full application layer.
Comparing Healthcare Website Development Stacks
Different practice sizes fit different development stacks. The table below shows the pattern that usually matches each practice type and the trade-off it accepts. Every stack has an honest downside. There is no universally best answer, only a best answer for a specific practice at a specific stage of growth.
| Practice size | Recommended stack | Monthly cost | Trade-off |
|---|---|---|---|
| Solo provider | WordPress on HIPAA host + booking widget | $50 to $150 hosting | Manual plugin updates |
| Small clinic (2 to 5 providers) | WordPress on managed HIPAA host | $150 to $400 | Plugin drift over time |
| Multi-location clinic | WordPress or specialty platform | $400 to $1,200 | Location-page maintenance |
| Specialty group (10+ sites) | Headless CMS + Next.js | $1,200 to $3,000 | Requires ongoing developer |
| DSO or hospital network | Custom stack with EHR integration | $3,000 plus | Long build, high compliance cost |
Reading the table honestly
The monthly cost column is hosting plus core managed services. It does not include the marketing retainer, the ongoing content work, or the paid campaigns. Practices that see the hosting number and assume it is the total cost end up under-budgeted for the site’s real operational envelope. Best-in-class scoping separates the build cost, the hosting cost, and the marketing retainer into three transparent line items so the practice can plan for the actual year-one number, not the launch-week number. The build cost is a one-time investment. Hosting is monthly. The marketing retainer is monthly and grows with the site. When those three numbers are stacked honestly at the scoping meeting, the practice can decide which stack fits the budget without discovering the total cost the hard way in month four.
Security, Forms, and Analytics in Healthcare Development
Security in healthcare development is not a checklist you tick after launch. It is a set of decisions embedded in the form stack, the analytics stack, the hosting configuration, and every third-party integration. Practices that miss any of them create the risk that shows up in state audit reports and news headlines. The three fastest-moving risk categories on healthcare sites are forms, analytics, and unpatched CMS installs.
Forms and the BAA question
Every form that collects protected health information needs an encrypted submission path, HIPAA-compatible storage, and a signed Business Associate Agreement with the vendor. Standard form plugins on default configurations do not qualify. The compliant options exist. They just have to be specified in the scope so the developer builds against the right stack. For a fuller view of the form security question, see our related Security Features for Healthcare Websites reference.
Analytics without capturing PHI
Standard analytics implementations on healthcare sites routinely capture URL parameters, form field content, or user identifiers that qualify as protected health information. The development side has to strip those signals at the tag manager, prefer server-side tagging where feasible, and audit the data layer regularly. A quarterly analytics audit that catches new exposure is a required part of the ongoing retainer, not a nice-to-have.
Patching cadence and unattended CMS installs
An unpatched WordPress install running out-of-date plugins is the single biggest source of healthcare site compromises. Every developer already knows this. Every practice still lets it happen because nobody was assigned the patching responsibility explicitly. The fix is boring. Assign the patching. Schedule it monthly. Log it.
Healthcare Web App Development and Real Integrations
Healthcare web app development lives at the intersection of scheduling systems, insurance platforms, EHR integrations, telehealth stacks, and payment processors. Each of those integrations has its own authentication model, data mapping, and compliance obligation. Most practices need only a subset. Getting the subset right at scoping saves months of rework at launch.
Scheduling integrations
Scheduling is the integration every practice needs. Options range from lightweight embed widgets like NexHealth or Zocdoc to deep API integrations with Epic MyChart or Cerner. The lightweight embeds cost less to build and less to maintain. The deep integrations offer better patient experience and lock the practice into the EHR vendor. Neither is universally right. The practice that already commits to an EHR usually needs the deep integration.
Insurance verification
Insurance verification on the public site removes the largest friction point in the booking flow. Real-time eligibility checks can be embedded via specialty vendors, but they require careful compliance work because the results are protected health information. Most solo practices ship a simpler pattern that surfaces the accepted payers and defers verification to the intake call. That is fine, and it avoids the compliance overhead.
Patient portal hand-offs
The public site rarely runs the patient portal. The public site hands off to the patient portal. That hand-off has to be smooth, authenticated, and clearly signposted. Patients who cannot find the portal login end up calling the office, which turns a self-serve interaction into a staff cost. Best-in-class development treats the portal hand-off as a first-class part of the site, not an afterthought footer link.
Healthcare Website Development Case Study From a Real Client
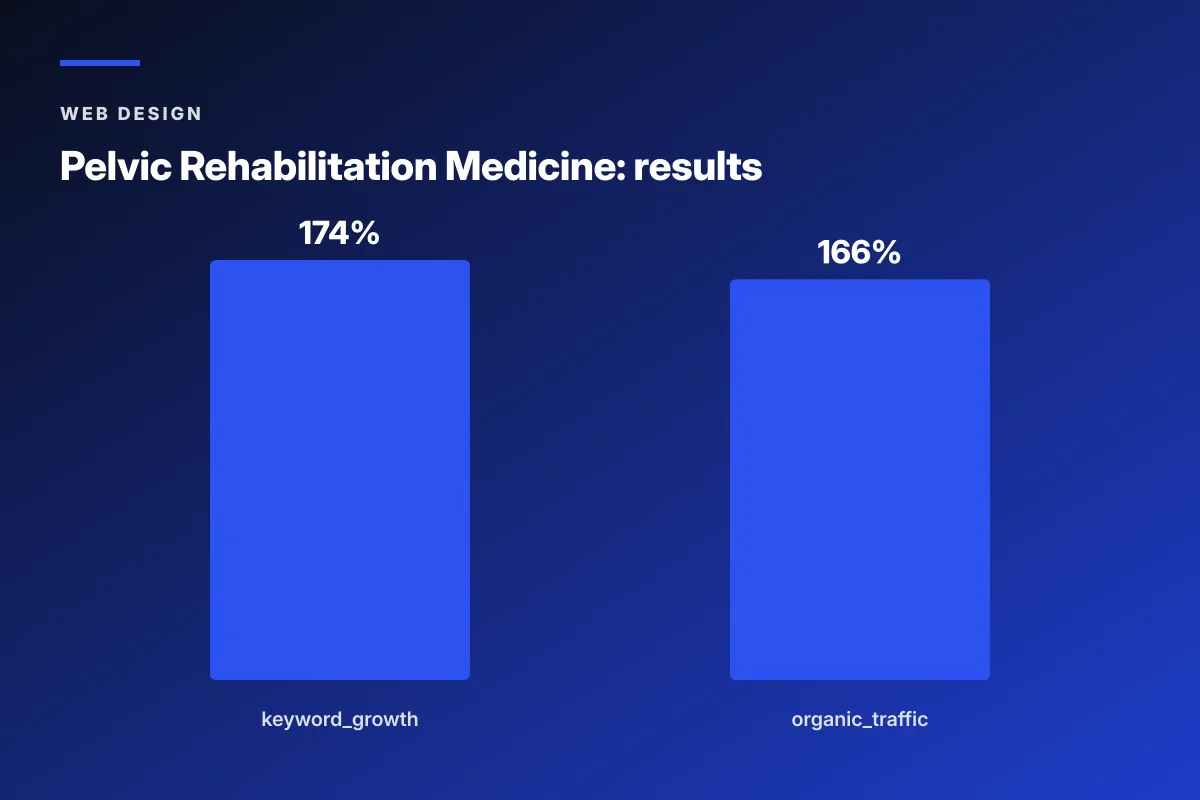
Pelvic Rehabilitation Medicine, a specialty medical group with 14 locations, engaged Redefine Web on a development project that had to scale a fragmented site into a working platform across a growing footprint. The development side handled a WordPress rebuild on a HIPAA-compliant host, a restructured URL architecture for location and condition pages, an accessibility remediation pass, and the launch of a dedicated patient community platform. Over the 2023 to 2024 engagement, organic keyword rankings expanded 174 percent year over year and organic traffic grew 166 percent, which validated the development-side decisions as much as the design ones.
Why the URL architecture change moved the number
The pre-project URLs mixed location and condition information in an inconsistent structure that search engines could not cleanly index. The development team restructured to a predictable pattern with condition-first URLs and location-first URLs handled by separate templates. That change alone let organic search finally surface the right pages for the right queries, without the copy having to change.
Why the community platform belongs in development scope
The patient community platform is a discrete piece of custom development that lives inside the broader site. Practices that want a community feature often assume it is a plugin. It rarely is. It usually requires custom moderation tools, spam mitigation, and privacy-aware user profile handling. Scoping it as a development project rather than a plugin decision was the reason it launched cleanly.
Hosting, Backups, and Ongoing Development
Hosting decisions get made once and pay recurring costs forever. Healthcare hosting is not the place to save money on the launch quote. The savings almost always come back as unexpected performance issues, uncovered PHI incidents, or plugin conflicts that a properly managed HIPAA host would have caught. For the deeper hosting-side discussion, see our related Healthcare Web Hosting reference.
What HIPAA-compliant hosting actually means
HIPAA-compliant hosting means the host signs a Business Associate Agreement, provides encryption at rest and in transit, offers audit logs, and runs the environment in a way that supports the practice’s own HIPAA obligations. Cheap shared hosting does not qualify. Managed HIPAA hosting with a signed BAA is a baseline expense, not a premium one, and it typically runs 150 to 500 dollars a month for a small practice.
Backups nobody checks
Backups run automatically at most hosts. They also fail silently at most hosts. A backup that has never been restored is not a backup. Every healthcare site should run at least a quarterly restore test to a staging environment to confirm the backup actually works and the restore procedure actually completes. This is boring work. It is also the difference between a bad afternoon and a bad year.
The one hosting joke every developer tells
The best-performing website is the one that stayed up during a state audit. Nobody wants to admire the uptime graph on a Monday, and everyone wants it on a Friday afternoon. Best-in-class hosting is invisible until it is not. That is the correct order for the invisibility to run in.
Performance Budgets and Core Web Vitals in Development
Performance in healthcare development is not something the developer optimizes after launch. It is a budget locked at the start of the build. Every asset the site loads has to fit inside a performance budget that keeps Largest Contentful Paint under 2.5 seconds on mobile at the 75th percentile of the practice’s real traffic. Development teams that lock this budget on day one hit the target. Teams that plan to optimize later almost never catch up. For the deeper Vitals view, see our related Core Web Vitals reference.
The image budget
Image weight is the largest single factor in healthcare site performance. A working budget sets a per-image ceiling of about 80 kilobytes for content images and 150 kilobytes for hero images, all served in WebP with responsive sizes. Practices that launch a site with 3-megabyte hero backgrounds inherit a permanent LCP problem that requires ongoing engineering to fix.
The third-party script budget
Every third-party script the practice adds costs a fraction of the performance budget. Chat widgets, review widgets, insurance verification embeds, and analytics tags all compound. A working budget caps the number of blocking third-party scripts at three, defers everything else, and reviews the list quarterly.
The font budget
Custom fonts eat performance budget. Best-in-class development limits the site to at most two custom font families, uses variable fonts where possible, preloads the critical fonts, and specifies matched fallback metrics to keep Cumulative Layout Shift below 0.1. Font decisions made in design without a matching development budget are the number one Vitals killer we see at launch.
How to Scope Healthcare Website Development Correctly
Scoping healthcare website development correctly is a project management skill more than a technical one. The developer has to ask the questions that reveal the integrations, the compliance obligations, and the maintenance model before the quote goes out. If those questions do not appear in the discovery call, the quote will be wrong.
- Which scheduling system, EHR, and patient portal does the practice already use.
- How many locations and how many providers are on the site today, and 24 months out.
- Who owns HIPAA compliance internally, and which vendors already have signed BAAs.
- What is the practice’s internal capacity for content updates without a developer.
- What is the current site’s performance baseline and what did the last audit find.
- What accessibility issues has the practice already had flagged.
- What is the year-one budget for hosting, maintenance, and ongoing development.
Why these questions shape the quote
Every answer changes the scope. A practice on Epic MyChart needs a different integration story than a practice on Zocdoc. A practice with no internal content capacity needs a CMS that non-technical staff can update. A practice with a bad accessibility audit history needs remediation baked into the build rather than tacked on later. The quote is not one number. It is a stack of decisions, each of which shifts the total.
Timelines that hold up
A realistic development-phase timeline for a mid-size healthcare site runs 10 to 16 weeks after design finalizes. Solo practice refreshes can finish in six weeks. Multi-location networks or specialty groups with EHR integrations take four to six months. Timelines under four weeks are either tiny scopes or missed compliance work. Timelines over eight months without staged deliverables usually indicate scope drift that will keep growing.
What happens after launch
Launch is halftime, not the finish. The first 30 days after launch are when analytics reveal the highest-friction points in the booking flow, when performance regressions show up under real traffic, and when the plugin and CMS ecosystem gives out its first updates. A working development contract includes at least 30 days of post-launch iteration bundled in the scope. Practices that treat launch as the finish line inherit a slowly degrading site.
Healthcare website development is where the site earns its long-term viability. For deeper reading, see the HHS HIPAA Security Rule, the Google Core Web Vitals documentation, and the WordPress developer security handbook. If your development quote has skipped any of the ten common requirements above, ask for a revised scope before you sign. If your team wants a working audit of a current healthcare site’s development quality against the standards in this piece, our team runs paid diagnostics that end in a prioritized fix list. For the design-side companion reference, see our Healthcare Web Design (Pillar).
Frequently asked questions
What does healthcare website development actually cover?
Healthcare website development covers everything behind the design. CMS setup, form architecture, hosting configuration, security hardening, third-party integrations, accessibility implementation, performance budgets, analytics setup, and QA passes. Each of those items is a design constraint in disguise, and every skipped item shows up as a bug three months after launch. Practices do not need to become experts in every layer, but they do need to understand which decisions live in the development phase because most expensive mistakes are made there. Discovery calls that skip these categories produce quotes that will be wrong by month two of the build.
How much does healthcare website development cost?
Healthcare website development projects run from around 6,000 dollars for a solo-provider WordPress build on a HIPAA host to 100,000 dollars or more for a multi-location specialty group with EHR integrations, custom patient portal work, and full accessibility remediation. The variables that push the number are the number of locations, the number of provider bios, whether the booking system stays or moves, whether custom application logic is required, and how much accessibility remediation the current site needs. Practices that under-scope QA, security, and compliance work usually pay a second time within a year.
How long does healthcare website development take?
A solo-provider refresh takes four to six weeks. A mid-size multi-provider clinic runs 10 to 16 weeks after design finalizes. Multi-location networks and specialty groups with EHR integrations run four to six months, sometimes longer if the integration vendors have their own certification timelines. Timelines under four weeks are almost always skipping accessibility QA, security hardening, or performance work. Timelines over eight months without staged deliverables usually indicate scope drift that will keep growing. Best-in-class projects launch in phases so revenue-generating pages go live early while iteration continues on the rest.
What is the difference between healthcare web development and healthcare web application development?
Healthcare web development builds the marketing site with service pages, provider bios, and a booking form that hands off to an external scheduling system. Healthcare web application development builds custom patient portals, appointment reminder systems, telehealth waiting rooms, and provider dashboards that involve custom application logic. Most single-provider and small multi-provider practices only need the marketing site. Multi-location networks, specialty groups with custom clinical workflows, and DSO operators typically need application-level work. Confusing the two categories at scoping is where budgets triple without a matching gain in outcomes for the practice.
What CMS is best for healthcare websites?
The best CMS for a healthcare website is the one that matches the practice's internal capacity for updates, integration needs, and available developer support. WordPress on a HIPAA-compatible managed host suits solo through mid-size practices with the widest plugin ecosystem and developer pool. Headless setups with Next.js suit multi-location specialty groups that need advanced performance and integrations and can afford a monthly developer retainer. Specialty healthcare platforms like Officite or MyAdvice suit smaller practices without internal technical staff who prefer to trade flexibility for a fully managed compliance stack. Picking the CMS the developer prefers rather than the CMS that fits the practice is the most common scoping mistake.
What are the security requirements for healthcare websites?
Healthcare websites need HIPAA-compliant hosting with a signed Business Associate Agreement, encrypted form submission with a BAA-covered form vendor, analytics that does not capture protected health information, monthly CMS and plugin patching, a web application firewall, rate limiting on login endpoints, regular user role audits, off-site encrypted backups with tested restores, and quarterly security scans. Every one of those items is a baseline requirement, not a premium add. Practices that skip any of them create risk exposure that shows up in state audit reports and news headlines. Assign every requirement to a named owner during scoping.
Book your free 30-minute strategy call.
No spam, no sales rep. We use your email to schedule your call with a senior strategist. That is it.
More from the blog
View all articles → Web Design
Web Design Core Web Vitals Healthcare Websites Actually Need to Book Patients
Read article Web Design
Web Design Professional Services Website Design Best Practices for 2026
Read article Web Design
Web Design