What Is a DSO in Dental and How It Works
- A DSO owns the non-clinical side of a dental practice.
- Management fees run 15 to 25 percent of collections.
- DSOs run about 30 percent of the US dental market in 2026.
- Equity rollover is the real return on affiliation.
- Per-location marketing is not optional at DSO scale.
- What is a DSO in dental care in one clean answer
- Dental service organization structure across the org chart
- What is a dental DSO doing behind the front desk
- Revenue splits for what is a dso in dental office deals
- The honest pros and cons of the dso dental structure
- A dental DSO case study that shows how the model runs at scale
- DSO meaning dental owners often mix up with corporate dentistry
- How many DSOs exist and how fast is the space growing
- Is a DSO the right move for your dental practice
- Marketing a dental DSO to fill schedules across every office
- Where to start if you are studying the DSO question for your own practice
What is a dso in dental practice, and why is every third piece of dental industry news for the last four years about them. A DSO is a Dental Support Organization. It owns the non-clinical side of a dental practice or a group of practices, handles the back office, and lets the dentist focus on chair time. You are looking at a business model that runs roughly 30 percent of the US dental market in 2026 and buys a new practice somewhere in the country almost every business day.
This guide is the honest read on what is a dso in dental terms. You get the structure, the ownership math, the revenue split, what a DSO takes off your plate, what it never touches, and the tradeoffs that decide whether joining one is right for your practice. You also get the marketing stack real DSOs run across locations, the case-study numbers behind it, and the questions to ask before signing. Read straight through in about ten minutes.

What is a DSO in dental care in one clean answer
A DSO is a Dental Support Organization. It runs the non-clinical side of one or more dental practices. Marketing, billing, HR, IT, procurement, compliance, and finance sit inside the DSO. Clinical decisions and the dental license stay with the dentist. That split defines the whole model.
The DSO signs a Management Services Agreement with each affiliated practice. Under that agreement, the DSO provides business services and takes a management fee, often 15 to 25 percent of collections. The dentist owns the professional entity that holds the license and the patient records. That structure keeps the model legal in the 30-plus states that require dentists to own dental practices, and it also creates the friction points that make DSO life either a dream or a nightmare depending on which DSO you sign with.
Who owns what inside a DSO
Ownership inside what is a dso in dental setup splits cleanly. The DSO owns the equipment, the office lease, the practice management software, the marketing accounts, the phone system, and every dollar of accounts receivable. The dentist owns the clinical entity, the license, the treatment plan, and the doctor-patient relationship. In most affiliation deals, the selling dentist rolls a portion of proceeds into equity in the DSO parent, keeping them tied to the group’s growth. In pure employment models, the associate dentist owns none of it and earns a salary plus production bonus. Read the affiliation contract twice before you sign it. See the ADA News archive for how these deals typically get structured.
Why the model works for both sides
The math on what is a dso in dental partnerships lands in favor of both sides once you scale. The DSO pools purchasing power, so a single office pays 30 percent less on supplies and 40 percent less on insurance. The dentist stops running payroll on a Sunday night. The DSO gets a growing revenue stream and a real portfolio of practices with clinical outcomes. The dentist gets time back and support that a solo practice cannot afford to build. Both sides win when the DSO respects clinical judgment. Both sides lose when the DSO pushes production targets that override care. That single tension defines the whole industry conversation.
Dental service organization structure across the org chart
The structural answer to what is a dso in dental terms starts with a two-layer org chart. A dental service organization runs a two-layer structure. The top layer is the corporate DSO, funded by private equity or by dentist founders, staffed with a CEO, a Chief Dental Officer, VPs of operations, marketing, HR, and finance, and often a growth team focused on acquiring new practices. The bottom layer is a network of practice PCs, each held by a licensed dentist and each linked to the DSO through a management services agreement. A mid-size DSO with 50 practices might carry 40 corporate staff and 400 clinical staff across the network.
Regional managers sit between corporate and the offices. Each regional lead runs 8 to 20 practices, visits each one on a rotation, handles operational escalations, and rolls up numbers to the executive team weekly. That layer is the difference between a DSO that feels like a real partner and one that feels like a call center that stopped answering the phone. Ask any dentist inside a DSO about their regional manager, and you learn everything you need to know about how the DSO actually runs day to day.
| Layer | Owns | Handles | Reports to |
|---|---|---|---|
| Corporate DSO | Brand, systems, capital | Marketing, HR, IT, procurement | Board and investors |
| Regional manager | Nothing | Ops across 8 to 20 offices | VP of operations |
| Practice PC | License, records, clinical calls | Patient care and production | Owner dentist and regional |
| Owner dentist | Professional entity | Clinical work, team leadership | Self plus DSO agreement |
The legal structure behind the split
Most states require a dentist to own any entity that practices dentistry. So the practice PC stays licensed to the dentist. The DSO parent is an LLC or a corporation with no clinical licensure. The management services agreement bridges the two entities and defines every service the DSO provides plus every fee the practice pays. Corporate practice of dentistry laws vary by state, and a DSO operating in 12 states writes 12 slightly different agreements. Get an attorney familiar with your state’s rules to read your contract before you sign it.
Where the money comes from
Most modern DSOs run on private equity capital. A PE firm buys a platform DSO with 8 to 15 practices, funds an acquisition team, buys 30 more practices over three years, and sells the whole thing to a bigger PE firm at a higher multiple. That cycle is called a roll-up. Some DSOs still run on dentist ownership, and a small number are cooperatives. The funding source shapes the culture. PE-backed DSOs push growth and production. Dentist-led DSOs move slower but often make better clinical calls. Ask which model funds the DSO courting you.
What is a dental DSO doing behind the front desk
A dental DSO runs a bundle of services the corporate parent delivers to every affiliated office. Marketing, billing, HR, IT, compliance, and procurement all sit in central teams. Practice-level staff stop doing back-office work and focus on chair time. The management fee pays for the bundle.
Marketing runs from a central team that handles brand, paid ads, local SEO, and website work across every location. Billing runs through a central RCM group that codes claims, chases denials, and posts payments. HR handles hiring, benefits, and payroll. IT keeps the practice management software, the phones, and the network humming. Compliance keeps HIPAA and OSHA in order. Procurement gets a bulk discount from Henry Schein or Patterson.
The value the practice receives is real. A solo office pays $60,000 to $120,000 a year for a full-time practice manager who does half those jobs poorly. The DSO delivers all of them at scale for a management fee that lands in the same range. That is the honest math on why the model spread so fast. Where it breaks is the DSO that promises the full stack and delivers half of it, or the DSO that centralizes marketing and forgets to run local map pack work for each office. If you are joining one, ask to see three months of marketing reports for practices your size before you sign.
The marketing stack a DSO actually runs
A working DSO marketing stack covers a shared brand site with per-location subpages, a Google Business Profile for every office, local SEO citations kept in sync, paid search built at the location level, paid social for awareness across the market, and a call tracking layer that ties every new patient back to the source. For a full breakdown, see our dental SEO services writeup, which covers the map pack work a DSO should never let slip.
The RCM and billing side you never think about
Revenue cycle management inside a DSO carries roughly 40 percent of the value the model delivers. Central RCM teams code claims correctly the first time, chase insurance denials with a scripted follow-up cadence, post payments daily, and reconcile every account monthly. A solo practice loses 4 to 8 percent of collections to bad coding and slow follow-up on denied claims. A DSO with a real RCM function pulls that number under 2 percent. Multiply that across 30 practices and the savings pay for the entire regional management layer.
Every DSO deal lives in the Management Services Agreement. Ask for the current MSA template on call one. If they won't send it, you're not close enough to talk.
Revenue splits for what is a dso in dental office deals
How a dso in dental office sends money up the chain is the single most important number to understand before you sign anything. The DSO takes a management fee, usually 15 to 25 percent of collections, sometimes structured as a fixed dollar amount plus a percentage. That fee covers everything the DSO provides. Doctor compensation gets set by contract, often 30 to 35 percent of collections for owner dentists in an affiliation deal, or a flat salary plus 25 to 30 percent production bonus for associates. Overhead runs 35 to 45 percent depending on region, insurance mix, and specialty focus.
Do the math on a $2 million practice. The DSO takes $400,000 in management fees. Overhead consumes $800,000. The owner dentist pulls $600,000 in comp plus equity in the parent. That equity number is where the real DSO return sits. On paper the dentist earns less than a comparable solo owner. On paper. The equity in the parent DSO becomes real money on the next PE recap, often two to five times the annual comp difference. Which is why every affiliation deal needs a qualified transaction attorney sitting next to the dentist at signing.
Management fee math worked out
A 20 percent management fee on a $2 million practice equals $400,000 per year to the DSO. That fee covers marketing, billing, HR, IT, procurement, compliance, real estate support, finance, and the regional operations layer. If those services would cost you $350,000 on your own with worse execution, the fee is fair. If those services would cost you $180,000 on your own with the same execution, the DSO is expensive. Get an itemized value list from the DSO before you sign. Vague answers on this question are the top warning sign.
Equity rollover as the real return
Most DSO affiliation deals ask the selling dentist to roll 20 to 40 percent of proceeds into equity in the DSO parent. That equity gets locked for two to five years while the DSO scales, then gets sold on to a larger PE firm at a higher enterprise value multiple. If the DSO doubles in size and sells at a 12x EBITDA multiple after buying at 8x, that rolled equity might return 2.5x. If the DSO struggles, the equity is worth what the buyer says it is worth. Ask about the parent’s growth trajectory, the current multiple, and the exit horizon before you touch the paperwork.
The honest pros and cons of the dso dental structure
The dso dental structure delivers benefits every solo dentist would like at some point in their career. Payroll, hiring, insurance credentialing, and CE reimbursement stop being your problem. Purchasing power drops supply costs 20 to 35 percent. Marketing shows up on a monthly report instead of getting invented on your kitchen table. Practice management software gets patched by someone else. If you sold to affiliate, you get liquidity that lets you buy a second house, pay for private school, or retire debt without waiting for a solo exit at retirement.
The tradeoffs are real too. Clinical autonomy gets pressured when the regional manager wants a certain production number. Team members you hired sometimes leave because a DSO benefits package still cannot match the culture you built as an owner. The dashboard the DSO shows you every Monday has KPIs you never used to track, and someone at HQ has an opinion on every one of them. Practice sale multiples in your market get set by the DSO buyer, and if you skip the affiliation window your solo exit price often lands 20 to 30 percent lower. See HubSpot on multi-location marketing for the operational tension every group runs into.
- Faster growth capital and access to a real acquisition team
- Purchasing power on supplies and lab work
- Central marketing plus per-location paid media
- Real HR, IT, and compliance behind you
- Liquidity event at sale plus equity upside
- Less time on payroll and vendor management
- Clinical decisions still yours on the operatory floor
The cons the sales team never leads with
Loss of true autonomy is the number one complaint on any dentist forum thread about DSO life. You still make clinical decisions, but a regional manager may push a production quota that ignores that a particular week ran heavy on hygiene checks. Team turnover often ticks up in the first six months of an affiliation as your best assistant realizes the DSO benefits package trades on scale, not on the culture you built. The management fee never adjusts down if collections dip. And your marketing team lives in another state and does not know that Mrs. Rogers on 4th Ave is the referral source that keeps the schedule full.
The pros that get real once you scale
Owning three practices as a solo dentist is a full-time operations job on top of chair time. Owning three practices inside a DSO is chair time plus quarterly strategy meetings. The math on your calendar shifts a lot the moment you cross practice number two. If your five-year plan involves growth beyond a single office, a DSO makes that plan possible with capital and infrastructure a solo path cannot match. If your plan is to run one great office until retirement, the DSO offers less and the tradeoffs sit heavier.
A dental DSO case study that shows how the model runs at scale
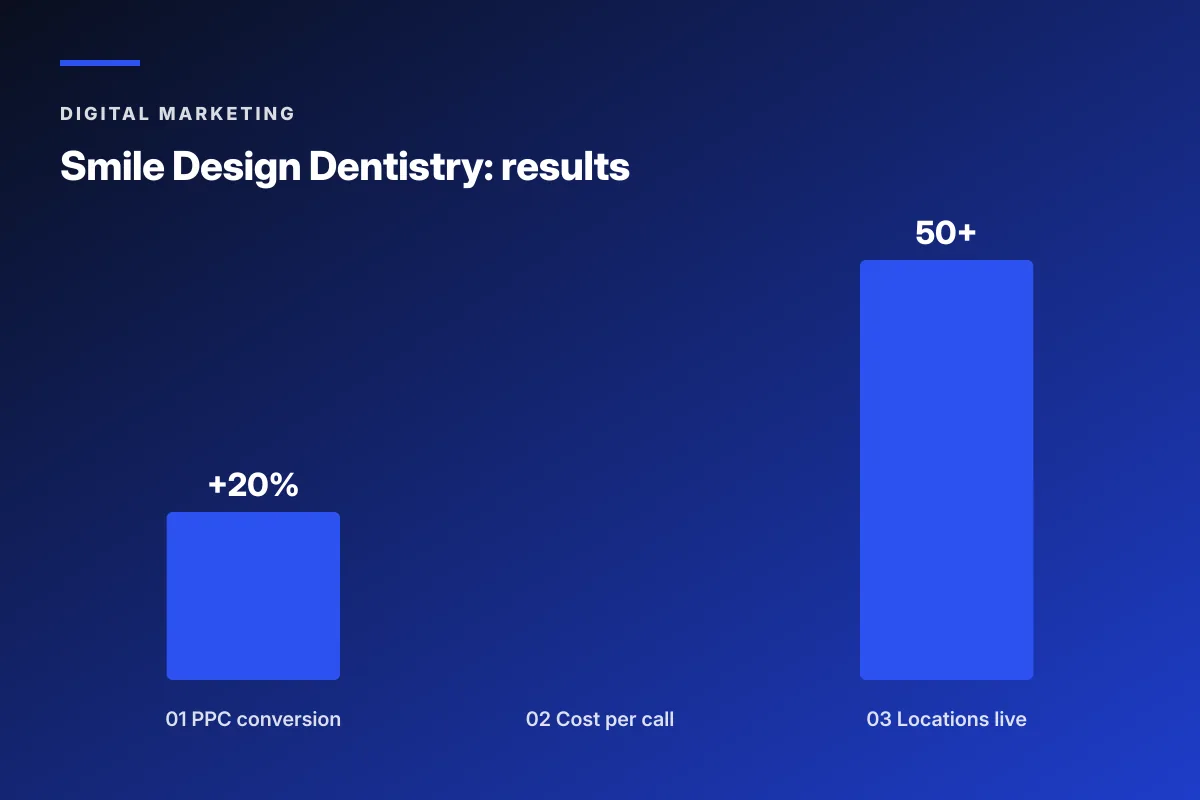
Smile Design Dentistry, a 50-plus location DSO based in Central Florida and Tampa Bay, came to us with a marketing problem that shows up in every mid-size DSO. Ad spend went up. Patient quality did not follow. PPC campaigns targeted too broadly, generated leads that rarely booked, and pushed acquisition costs into the wrong side of the P and L. Social was underused. Tracking was thin enough that the executive team could not tell which office pulled the strongest paid media performance in any given month.
We ran a per-location, per-funnel-stage rebuild. Google Ads got restructured by geo and by intent stage. Landing pages got built for each office with local trust cues layered under a national brand system. CallRail integration scored every call by patient quality, not just call volume. Paid social launched with awareness, consideration, and conversion layers built to move a prospect through the funnel with video and demographic precision. PPC conversion rate gained 20 percent. Cost per call dropped 30 percent. All 50-plus offices got optimized campaigns instead of a shared template.
What worked inside the rebuild
Segmenting campaigns by funnel stage cut waste on the search side by routing high-intent clicks to the right offices with capacity. Local landing pages carried the same brand system as the parent but named the neighborhood, the front office manager, and the two closest cross streets. Every phone call scored on booked or not booked, which turned the paid media dashboard from a vanity report into a decision tool. Weekly reporting by office let the executive team push budget to the highest-performing markets instead of splitting spend equally across 50 markets that never performed equally.
What carried over to other DSOs on the same stack
The Smile Design playbook translates cleanly to any DSO running 10-plus offices in a shared media market. Per-location landing pages with local trust cues, call scoring on every ring, funnel-stage campaign structure, and weekly per-office reporting are the four pieces that force real accountability into a group marketing program. Skip any one of them and the paid media budget grows every quarter without moving new patient counts. Study our DSO dental marketing for multi-location groups writeup for the full rollout pattern.

Every DSO recruiting pitch to a solo owner follows the same script. The rep smiles. They say partnership. They say growth. They pull out a slide with a bar chart. The bar chart is always going up and to the right. They mention the word autonomy nine times in ninety minutes. They leave you with a term sheet and a coffee mug. The mug is fine. Then you read the term sheet at 11 pm on a Tuesday, realize the management fee applies to gross collections not net, and spend the next two weeks trying to reach the rep who has stopped returning calls.
DSO meaning dental owners often mix up with corporate dentistry
The dso meaning dental owners often use interchangeably with corporate dentistry is not quite right. Corporate dentistry is a broader category that includes DSOs, publicly traded chains, insurance-owned practice groups, and private equity platforms. A DSO is one specific model inside that category. Every DSO is corporate dentistry. Not every corporate dental group is a DSO. The distinction matters when reading industry news, when comparing acquisition offers, and when explaining to your team what actually changed after you affiliated.
The legal test is the management services agreement. If the corporate parent owns and operates every practice directly, that is a chain, not a DSO. If the corporate parent runs business services under an MSA with a licensed dentist who owns the practice PC, that is a DSO. That structural detail decides how the model works in states with strict corporate practice laws. It also decides the answer to which party can sell the practice, hire the dentist, and terminate the affiliation.
Chain vs DSO in one paragraph
A dental chain owns every office and employs every dentist as W-2 staff. A DSO keeps clinical ownership in the hands of the licensed dentist and runs business services from the outside. Chains ran the corporate dentistry model in the 1990s. DSOs replaced them starting in the mid-2000s once state dental boards pushed back on chain ownership. Today the DSO model dominates because the structure keeps the corporate practice laws happy and gives the dentist enough clinical control to keep the state board off their back. Small difference. Huge legal impact.
DSO vs a plain group practice
A group practice is a partnership between two or more dentists who share overhead, staff, and a location or two. No corporate parent. No management fee. No outside investors. The group is the operating entity. A DSO layers a business support company on top of practices owned by different dentists, funded by outside capital, and coordinated through central operations. Group practices tap out at three to five offices before the operations get impossible. DSOs scale past 500 offices because the corporate layer absorbs the operational load that would kill a partnership.
How many DSOs exist and how fast is the space growing
Roughly 400 to 500 DSOs run in the US in 2026, covering about 12,000 to 14,000 dental practices, close to 30 percent of the market. Five years ago the number sat at 18 percent. Growth runs on private equity capital and on solo dentists reaching retirement with fewer buyers among younger graduates.
Growth is driven by two forces. First, private equity capital keeps funding platform DSOs and roll-up acquisitions. Second, solo dentists reaching retirement have fewer buyers among younger dentists carrying student loans, which pushes them toward a DSO exit. The two forces reinforce each other and neither is slowing.
Big DSOs get most of the coverage. Heartland Dental runs about 1,700 offices. Aspen Dental Management runs about 1,000. Pacific Dental Services runs about 950. MB2 Dental, Smile Brands, and Great Expressions each run several hundred. But the tail is long. The typical DSO you might join runs 15 to 60 offices, sits under a mid-market PE firm, and plans to sell to a larger PE firm inside five years. That mid-tier segment is where most affiliation deals happen and where the equity rollover math actually delivers if the timing goes right.
Platform DSO vs a tuck-in acquisition
A platform DSO is the first practice or small group a PE firm buys to anchor a roll-up. Platform multiples run higher because the buyer is also buying the executive team and the operating model. A tuck-in acquisition is a smaller practice added to an existing platform. Tuck-in multiples run lower because the buyer already has infrastructure. Solo owners usually get tuck-in economics unless they carry unusual features, like specialty focus, high production per chair, or a strategic geography the platform needs. Know which side of that line you sit on before you name a number.
Specialty DSOs are the fastest-growing segment
Orthodontics, pediatric dentistry, oral surgery, and endodontics each have specialty DSOs consolidating that segment faster than general dentistry consolidated a decade ago. Smile Doctors runs the largest ortho DSO with several hundred offices. Pediatric platforms like Smile Design and Chompers scale similar rollups on the pediatric side. Specialty DSOs pay higher acquisition multiples because the referral flow, the case value, and the payer mix each carry more predictable economics than a general practice. A specialist thinking about affiliation should ask for specialty comparables, not general dentistry data.
Is a DSO the right move for your dental practice
A DSO fits when three answers line up. Retirement sits inside a decade. Growth past one location matters to you. And losing 15 percent of operational calls to a regional manager will not wreck your Monday. Miss any one of those and affiliation gets rocky fast.
The last question on what is a dso in dental terms for your own practice: whether a DSO fits your practice depends on three questions. First, how long do you plan to keep practicing chairside. If retirement sits inside a decade, the DSO affiliation timing matches your exit. Second, do you want to grow past a single location. If yes, DSO capital moves you faster than solo growth. Third, how much clinical autonomy do you need to stay happy. If losing 15 percent of operational calls to a regional manager would ruin your Monday morning, you will not survive an affiliation, no matter how good the term sheet reads.
Practices most likely to be happy inside a DSO are producing $1.5 million to $6 million a year, run three or fewer operatories, want out of operational headaches, and have an owner within ten years of retirement. Practices most likely to regret a DSO deal are producing under $900,000, run heavy specialty procedures the DSO does not staff for, or have a strong personal-brand owner whose patients would not stay after the sale. The fit question is not about the DSO. It is about the practice.
- Practice production between $1.5M and $6M annually
- Owner within 10 years of retirement or seeking growth capital
- Team open to a benefits and operations change
- Payer mix that matches the DSO’s target
- Real estate the DSO wants long-term
- Clinical protocols compatible with DSO standards
Questions to answer before you call a DSO
Read your last three years of tax returns before you talk to a DSO. Know your EBITDA. Know your collections trend. Know your patient count. Know your production per hour. Know your insurance write-off percentage. If you cannot recite those numbers, you are not ready to negotiate. DSO reps are trained to walk you through their preferred multiple. Your preparation is the only counterweight. Get your accountant to run a quality-of-earnings analysis before you sign anything. That report costs about $8,000 and saves ten times that in the negotiation.
What to expect after you say yes
The first 90 days after closing are the hardest. The DSO drops its operating manual on your team. Your practice management software may switch. Your uniforms may change. A regional manager visits every week. Some team members quit. Others rise. Marketing budget moves from your local vendor to the DSO central team. Patient reactions vary. Most patients notice nothing. Some ask why the front desk voicemail changed. Give the transition a full year before you judge the deal. The rough patches usually smooth out. The permanent changes are worth knowing about in advance.
Marketing a dental DSO to fill schedules across every office
Marketing a DSO is a different discipline than marketing a solo practice. A DSO runs shared brand equity across many locations, and every location competes for the local map pack, paid search geo, and review reputation on its own patch. Central marketing teams that treat 40 offices as one market lose. Central marketing teams that build 40 local programs on a shared operational backbone win. That is the entire distinction between a DSO whose organic new patient count climbs every quarter and one whose paid budget grows without moving the schedule.
The stack that actually works pairs a shared brand with local Google Business Profile management, per-location SEO service pages, geo-targeted paid search built at the office level, awareness and consideration paid social layered across the market, and a call tracking layer feeding a central dashboard. That last piece decides whether the executive team can make budget decisions off real data. NC Dental Clinic, a Vista California practice that came to us before it was affiliated, followed the same template and posted 1,000 percent patient growth over the multi-year program. See our dental marketing agency hub for the full stack. For the retainer math, our dental marketing retainer covers what a real multi-location engagement runs. And Google Search Central is the reference for schema markup a DSO site should carry across every location page.
Per-location work is not optional
The single fastest way for a DSO to underperform its brand equity is a central marketing team that runs one campaign across every office. Local pack rankings live on office-specific GBP work, office-specific citations, and office-specific review flow. If the DSO cannot show you three months of per-office paid media reports on a call, the operation is running on autopilot and the offices you affiliate are footing the bill for that autopilot. Ask for the reports before you sign. The answer tells you everything.
Balancing brand equity with local trust
A patient searching for a dentist wants two things. A brand they recognize. And a real person who works at the office three miles from their house. The DSO carrying both wins. The DSO carrying only the brand loses to the solo office down the street with the loyal front desk manager. The DSO carrying only the local pieces looks scrappy but never captures the aided-recall gain a national brand delivers. The right stack layers both. A shared brand system on top of location-specific pages, staff bios with real photos, and reviews collected office by office. Neither piece is optional at scale.
Where to start if you are studying the DSO question for your own practice
Start with your numbers before deciding what is a dso in dental terms for your future. Pull three years of tax returns. Run a quality-of-earnings analysis. Then talk to three DSOs. Not one. Three. Compare the term sheets side by side. Look at the management fee, the equity rollover percentage, the doctor comp formula, the noncompete radius, and the exit terms. If two DSOs come in inside a 10 percent band, the deal is fair. If one is 25 percent above the others, ask why. If one is 25 percent below, walk. Talk to two dentists inside each DSO before you sign. Ask the hard questions off the record.
Then think about whether affiliation is the right move at all. Some practices grow faster and earn more staying solo. Some owners hate the operational load and would trade 10 percent of lifetime earnings to hand it off. Neither answer is wrong. Both answers require honest math. Ready to look at what a real dental marketing program covers, our dental PPC management writeup shows how paid media should be structured for a growth practice. For the SEO side, our dental SEO services covers the map pack work every DSO office needs.
Frequently asked questions
What is a DSO in dental practice and how does it work
A DSO is a Dental Support Organization that owns and operates the non-clinical side of a dental practice or a group of practices. Marketing, billing, HR, IT, compliance, procurement, and finance sit inside the DSO. The clinical work and the dental license stay with the licensed dentist who owns the practice PC. A management services agreement between the two entities defines the services the DSO provides and the fees the practice pays, usually 15 to 25 percent of collections. That split keeps the model legal under state corporate practice laws and lets the dentist focus on chair time while the DSO handles the operations.
What is a dental DSO paying for and what does it own
A dental DSO owns the equipment, the office lease, the practice management software, the marketing accounts, the phone systems, and the accounts receivable across every affiliated office. The DSO pays for marketing, billing, HR, IT support, compliance, real estate, and procurement out of the management fee, and it earns money on the fee itself plus growth in the enterprise value of the parent. The dentist owns the professional entity holding the license, the patient records, and the clinical judgment. That split is the entire point of the model. Legal, operational, and financial responsibility get divided cleanly between the corporate side and the clinical side.
What is the DSO meaning dental industry uses when they say corporate dentistry
The DSO meaning dental owners often confuse with corporate dentistry is not identical. Corporate dentistry is the umbrella term for any commercial ownership structure in dentistry, which includes DSOs, publicly traded chains, insurance-owned practice groups, and private equity platforms. A DSO is one specific model inside that category, defined by a management services agreement between a business entity and a dentist-owned practice PC. Every DSO is corporate dentistry. Not every corporate dental group is a DSO. The distinction matters when reading industry data, evaluating an acquisition offer, or explaining what changed after affiliation to your team, your patients, and your state dental board.
How much does a DSO in dental office arrangements pay the dentist
Doctor compensation inside a DSO depends on the role. Owner dentists in an affiliation deal usually earn 30 to 35 percent of collections plus equity in the DSO parent that vests over two to five years. Associate dentists on employment contracts earn a base salary of $150,000 to $220,000 plus a production bonus of 25 to 30 percent above a daily threshold. The compensation number by itself understates the deal. Owner dentists who roll equity often earn more on the recap event than they earn from annual pay over the same period. That equity return is the real math on why so many owners affiliate now rather than wait for a solo exit at retirement.
What is a dental service organization structure across the org chart
A dental service organization structure runs two layers. The corporate DSO sits at the top with a CEO, Chief Dental Officer, VPs of operations, marketing, HR, and finance, plus an acquisition team. The practices sit at the bottom, each a licensed dental PC owned by a dentist and linked to the corporate parent through a management services agreement. A regional manager layer bridges the two, with each regional lead covering 8 to 20 offices, visiting on rotation, and handling operational escalation. A 50-office DSO typically staffs 40 corporate employees against 400 clinical staff. The quality of the regional layer decides how the DSO feels day to day.
How do you tell a DSO office apart from a solo dental practice from the outside
Signals that a dental office belongs to a DSO include a corporate website that lists multiple locations under a shared brand, a phone system that routes to a central call center before reaching the office, a treatment plan discussion that references corporate treatment guidelines, benefits packages that name a national parent company for staff, and appointment scheduling handled by a shared team across offices. Some DSOs keep the original office name and add corporate infrastructure quietly behind the scenes, in which case the signal is a change in the front desk personnel, the software, or the review response tone. Ask the office directly. Most will tell you.
Book your free 30-minute strategy call.
No spam, no sales rep. We use your email to schedule your call with a senior strategist. That is it.
More from the blog
View all articles → Digital Marketing
Digital Marketing Dental Marketing Tips That Compound Into New Patients
Read article Digital Marketing
Digital Marketing Ecommerce Marketing Strategies That Drive Real DTC Revenue
Read article Digital Marketing
Digital Marketing